Gallstones
What are gallstones?
Gallstones are hard particles that develop in the gallbladder. The gallbladder is a small, pear-shaped organ located in the upper right abdomen—the area between the chest and hips—below the liver.
Gallstones can range in size from a grain of sand to a golf ball. The gallbladder can develop a single large gallstone, hundreds of tiny stones, or both small and large stones. Gallstones can cause sudden pain in the upper right abdomen. This pain, called a gallbladder attack or biliary colic, occurs when gallstones block the ducts of the biliary tract.
What is the biliary tract?
The biliary tract consists of the gallbladder and the bile ducts. The bile ducts carry bile and other digestive enzymes from the liver and pancreas to the duodenum—the first part of the small intestine.
The liver produces bile—a fluid that carries toxins and waste products out of the body and helps the body digest fats and the fat-soluble vitamins A, D, E, and K. Bile mostly consists of cholesterol, bile salts, and bilirubin. Bilirubin, a reddish-yellow substance, forms when hemoglobin from red blood cells breaks down. Most bilirubin is excreted through bile.
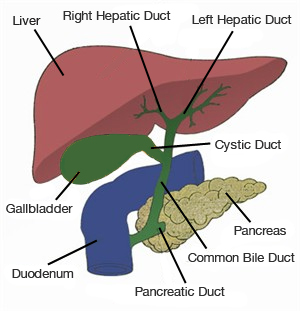
The bile ducts of the biliary tract include the hepatic ducts, the common bile duct, the pancreatic duct, and the cystic duct. The gallbladder stores bile. Eating signals the gallbladder to contract and empty bile through the cystic duct and common bile duct into the duodenum to mix with food.
What causes gallstones?
Imbalances in the substances that make up bile cause gallstones. Gallstones may form if bile contains too much cholesterol, too much bilirubin, or not enough bile salts. Scientists do not fully understand why these imbalances occur. Gallstones also may form if the gallbladder does not empty completely or often enough.
The two types of gallstones are cholesterol and pigment stones:
- Cholesterol stones, usually yellow-green in color, consist primarily of hardened cholesterol. In the United States, more than 80 percent of gallstones are cholesterol stones.
- Pigment stones, dark in color, are made of bilirubin.
Who is at risk for gallstones?
Certain people have a higher risk of developing gallstones than others:
- Women are more likely to develop gallstones than men. Extra estrogen can increase cholesterol levels in bile and decrease gallbladder contractions, which may cause gallstones to form. Women may have extra estrogen due to pregnancy, hormone replacement therapy, or birth control pills.
- People over age 40 are more likely to develop gallstones than younger people.
- People with a family history of gallstones have a higher risk.
- American Indians have genetic factors that increase the amount of cholesterol in their bile. In fact, American Indians have the highest rate of gallstones in the United States—almost 65 percent of women and 30 percent of men have gallstones.
- Mexican Americans are at higher risk of developing gallstones.
Other factors that affect a person’s risk of gallstones include
- Obesity. People who are obese, especially women, have increased risk of developing gallstones. Obesity increases the amount of cholesterol in bile, which can cause stone formation.
- Rapid weight loss. As the body breaks down fat during prolonged fasting and rapid weight loss, the liver secretes extra cholesterol into bile. Rapid weight loss can also prevent the gallbladder from emptying properly. Low-calorie diets and bariatric surgery—surgery that limits the amount of food a person can eat or digest—lead to rapid weight loss and increased risk of gallstones.
- Diet. Research suggests diets high in calories and refined carbohydrates and low in fiber increase the risk of gallstones. Refined carbohydrates are grains processed to remove bran and germ, which contain nutrients and fiber. Examples of refined carbohydrates include white bread and white rice.
- Certain intestinal diseases. Diseases that affect normal absorption of nutrients, such as Crohn’s disease, are associated with gallstones.
- Metabolic syndrome, diabetes, and insulin resistance. These conditions increase the risk of gallstones. Metabolic syndrome also increases the risk of gallstone complications. Metabolic syndrome is a group of traits and medical conditions linked to being overweight or obese that puts people at risk for heart disease and type 2 diabetes.
Pigment stones tend to develop in people who have
- cirrhosis—a condition in which the liver slowly deteriorates and malfunctions due to chronic, or long lasting, injury
- infections in the bile ducts
- severe hemolytic anemias—conditions in which red blood cells are continuously broken down, such as sickle cell anemia
What are the symptoms and complications of gallstones?
Many people with gallstones do not have symptoms. Gallstones that do not cause symptoms are called asymptomatic, or silent, gallstones. Silent gallstones do not interfere with the function of the gallbladder, liver, or pancreas.
If gallstones block the bile ducts, pressure increases in the gallbladder, causing a gallbladder attack. The pain usually lasts from 1 to several hours. Gallbladder attacks often follow heavy meals, and they usually occur in the evening or during the night.
Gallbladder attacks usually stop when gallstones move and no longer block the bile ducts. However, if any of the bile ducts remain blocked for more than a few hours, complications can occur. Complications include inflammation, or swelling, of the gallbladder and severe damage or infection of the gallbladder, bile ducts, or liver.
A gallstone that becomes lodged in the common bile duct near the duodenum and blocks the pancreatic duct can cause gallstone pancreatitis—inflammation of the pancreas.
Left untreated, blockages of the bile ducts or pancreatic duct can be fatal.
When should a person talk with a health care provider about gallstones?
People who think they have had a gallbladder attack should notify their health care provider. Although these attacks usually resolve as gallstones move, complications can develop if the bile ducts remain blocked.
People with any of the following symptoms during or after a gallbladder attack should see a health care provider immediately:
- abdominal pain lasting more than 5 hours
- nausea and vomiting
- fever—even a low-grade fever—or chills
- yellowish color of the skin or whites of the eyes, called jaundice
- tea-colored urine and light-colored stools
These symptoms may be signs of serious infection or inflammation of the gallbladder, liver, or pancreas.
How are gallstones diagnosed?
A health care provider will usually order an ultrasound exam to diagnose gallstones. Other imaging tests may also be used.
- Ultrasound exam. Ultrasound uses a device, called a transducer, that bounces safe, painless sound waves off organs to create an image of their structure. A specially trained technician performs the procedure in a health care provider’s office, outpatient center, or hospital, and a radiologist—a doctor who specializes in medical imaging—interprets the images. Anesthesia is not needed. If gallstones are present, they will be visible in the image. Ultrasound is the most accurate method to detect gallstones.
- Computerized tomography (CT) scan. A CT scan is an x ray that produces pictures of the body. A CT scan may include the injection of a special dye, called contrast medium. CT scans use a combination of x rays and computer technology to create three-dimensional (3-D) images. CT scans require the person to lie on a table that slides into a tunnel-shaped device where the x rays are taken. An x-ray technician performs the procedure in an outpatient center or hospital, and a radiologist interprets the images. Anesthesia is not needed. CT scans can show gallstones or complications, such as infection and blockage of the gallbladder or bile ducts. However, CT scans can miss gallstones that are present.
- Magnetic resonance imaging (MRI). MRI machines use radio waves and magnets to produce detailed pictures of the body’s internal organs and soft tissues without using x rays. A specially trained technician performs the procedure in an outpatient center or hospital, and a radiologist interprets the images. Anesthesia is not needed, though people with a fear of confined spaces may receive light sedation. An MRI may include the injection of contrast medium. With most MRI machines, the person lies on a table that slides into a tunnel-shaped device that may be open ended or closed at one end; some newer machines allow the person to lie in a more open space. MRIs can show gallstones in the ducts of the biliary system.
- Cholescintigraphy. Cholescintigraphy—also called a hydroxyl iminodiacetic acid scan, HIDA scan, or hepatobiliary scan—uses an unharmful radioactive material to produce pictures of the biliary system. In cholescintigraphy, the person lies on an exam table and a health care provider injects a small amount of unharmful radioactive material into a vein in the person’s arm. The health care provider may also inject a substance that causes the gallbladder to contract. A special camera takes pictures of the radioactive material as it moves through the biliary system. A specially trained technician performs the procedure in an outpatient center or hospital, and a radiologist interprets the images. Anesthesia is not needed. Cholescintigraphy is used to diagnose abnormal contractions of the gallbladder or obstruction of the bile ducts.
- Endoscopic retrograde cholangiopancreatography (ERCP). ERCP uses an x ray to look into the bile and pancreatic ducts. After lightly sedating the person, the health care provider inserts an endoscope—a small, flexible tube with a light and a camera on the end—through the mouth into the duodenum and bile ducts. The endoscope is connected to a computer and video monitor. The health care provider injects contrast medium through the tube into the bile ducts, which makes the ducts show up on the monitor. The health care provider performs the procedure in an outpatient center or hospital. ERCP helps the health care provider locate the affected bile duct and the gallstone. The stone is captured in a tiny basket attached to the endoscope and removed. This test is more invasive than other tests and is used selectively.
Health care providers also use blood tests to look for signs of infection or inflammation of the bile ducts, gallbladder, pancreas, or liver. A blood test involves drawing blood at a health care provider’s office or commercial facility and sending the sample to a lab for analysis.
Gallstone symptoms may be similar to those of other conditions, such as appendicitis, ulcers, pancreatitis, and gastroesophageal reflux disease.
Sometimes, silent gallstones are found when a person does not have any symptoms. For example, a health care provider may notice gallstones when performing ultrasound for a different reason.
How are gallstones treated?
If gallstones are not causing symptoms, treatment is usually not needed. However, if a person has a gallbladder attack or other symptoms, a health care provider will usually recommend treatment. A person may be referred to a gastroenterologist—a doctor who specializes in digestive diseases—for treatment. If a person has had one gallbladder attack, more episodes will likely follow.
The usual treatment for gallstones is surgery to remove the gallbladder. If a person cannot undergo surgery, nonsurgical treatments may be used to dissolve cholesterol gallstones. A health care provider may use ERCP to remove stones in people who cannot undergo surgery or to remove stones from the common bile duct in people who are about to have gallbladder removal surgery.
Surgery
Surgery to remove the gallbladder, called cholecystectomy, is one of the most common operations performed on adults in the United States.
The gallbladder is not an essential organ, which means a person can live normally without a gallbladder. Once the gallbladder is removed, bile flows out of the liver through the hepatic and common bile ducts and directly into the duodenum, instead of being stored in the gallbladder.
Surgeons perform two types of cholecystectomy:
Laparoscopic cholecystectomy. In a laparoscopic cholecystectomy, the surgeon makes several tiny incisions in the abdomen and inserts a laparoscope—a thin tube with a tiny video camera attached. The camera sends a magnified image from inside the body to a video monitor, giving the surgeon a close-up view of organs and tissues. While watching the monitor, the surgeon uses instruments to carefully separate the gallbladder from the liver, bile ducts, and other structures. Then the surgeon removes the gallbladder through one of the small incisions. Patients usually receive general anesthesia.
Most cholecystectomies are performed with laparoscopy. Many laparoscopic cholecystectomies are performed on an outpatient basis, meaning the person is able to go home the same day. Normal physical activity can usually be resumed in about a week.
Open cholecystectomy. An open cholecystectomy is performed when the gallbladder is severely inflamed, infected, or scarred from other operations. In most of these cases, open cholecystectomy is planned from the start. However, a surgeon may perform an open cholecystectomy when problems occur during a laparoscopic cholecystectomy. In these cases, the surgeon must switch to open cholecystectomy as a safety measure for the patient.
To perform an open cholecystectomy, the surgeon creates an incision about 4 to 6 inches long in the abdomen to remove the gallbladder. Patients usually receive general anesthesia. Recovery from open cholecystectomy may require some people to stay in the hospital for up to a week. Normal physical activity can usually be resumed after about a month.
A small number of people have softer and more frequent stools after gallbladder removal because bile flows into the duodenum more often. Changes in bowel habits are usually temporary; however, they should be discussed with a health care provider.
Though complications from gallbladder surgery are rare, the most common complication is injury to the bile ducts. An injured common bile duct can leak bile and cause a painful and possibly dangerous infection. One or more additional operations may be needed to repair the bile ducts. Bile duct injuries occur in less than 1 percent of cholecystectomies.
Nonsurgical Treatments for Cholesterol Gallstones
Nonsurgical treatments are used only in special situations, such as when a person with cholesterol stones has a serious medical condition that prevents surgery. Gallstones often recur within 5 years after nonsurgical treatment.
Two types of nonsurgical treatments can be used to dissolve cholesterol gallstones:
- Oral dissolution therapy. Ursodiol (Actigall) and chenodiol (Chenix) are medications that contain bile acids that can dissolve gallstones. These medications are most effective in dissolving small cholesterol stones. Months or years of treatment may be needed to dissolve all stones.
- Shock wave lithotripsy. A machine called a lithotripter is used to crush the gallstone. The lithotripter generates shock waves that pass through the person’s body to break the gallstone into smaller pieces. This procedure is used only rarely and may be used along with ursodiol.
Eating, Diet, and Nutrition
Factors related to eating, diet, and nutrition that increase the risk of gallstones include
- obesity
- rapid weight loss
- diets high in calories and refined carbohydrates and low in fiber
People can decrease their risk of gallstones by maintaining a healthy weight through proper diet and nutrition.
Ursodiol can help prevent gallstones in people who rapidly lose weight through low-calorie diets or bariatric surgery. People should talk with their health care provider or dietitian about what diet is right for them.
Points to Remember
- Gallstones are hard particles that develop in the gallbladder.
- Imbalances in the substances that make up bile cause gallstones. Gallstones may form if bile contains too much cholesterol, too much bilirubin, or not enough bile salts. Scientists do not fully understand why these imbalances occur.
- Women, people over age 40, people with a family history of gallstones, American Indians, and Mexican Americans have a higher risk of developing gallstones.
- Many people with gallstones do not have symptoms. Gallstones that do not cause symptoms are called asymptomatic, or silent, gallstones.
- If gallstones block the bile ducts, pressure increases in the gallbladder, causing a gallbladder attack.
- Gallbladder attacks often follow heavy meals, and they usually occur in the evening or during the night.
- Gallstone symptoms may be similar to those of other conditions.
- If gallstones are not causing symptoms, treatment is usually not needed. However, if a person has a gallbladder attack or other symptoms, a health care provider will usually recommend treatment.
- The usual treatment for gallstones is surgery to remove the gallbladder. If a person cannot undergo surgery, nonsurgical treatments may be used to dissolve cholesterol gallstones. A health care provider may use endoscopic retrograde cholangiopancreatography (ERCP) to remove stones in people who cannot undergo surgery or to remove stones from the common bile duct in people who are about to have gallbladder removal surgery.
- The gallbladder is not an essential organ, which means a person can live normally without a gallbladder. Once the gallbladder is removed, bile flows out of the liver through the hepatic and common bile ducts and directly into the duodenum, instead of being stored in the gallbladder.
References
Clinical Trials
The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) and other components of the National Institutes of Health (NIH) conduct and support research into many diseases and conditions.
What are clinical trials, and are they right for you?
Clinical trials are part of clinical research and at the heart of all medical advances. Clinical trials look at new ways to prevent, detect, or treat disease. Researchers also use clinical trials to look at other aspects of care, such as improving the quality of life for people with chronic illnesses. Find out if clinical trials are right for you
What clinical trials are open?
Clinical trials that are currently open and are recruiting can be viewed at www.ClinicalTrials.gov
This information may contain content about medications and, when taken as prescribed, the conditions they treat. When prepared, this content included the most current information available. For updates or for questions about any medications, contact the U.S. Food and Drug Administration toll-free at 1-888-INFO-FDA (1-888-463-6332) or visit www.fda.gov. Consult your health care provider for more information.
The U.S. Government does not endorse or favor any specific commercial product or company. Trade, proprietary, or company names appearing in this document are used only because they are considered necessary in the context of the information provided. If a product is not mentioned, the omission does not mean or imply that the product is unsatisfactory.
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts.
The NIDDK would like to thank:
Michael G. Sarr, M.D., Mayo Clinic
This information is not copyrighted. The NIDDK encourages people to share this content freely.
November 2013